About Forwardontics
Forwardontics is a descriptive term for the general public and includes all treatments that focus on forward development of teeth and jaws in both children and adults. Forwardontics, in contrast to the remainder of orthodontics, focuses on the face and the causes of malocclusion. It is most often practiced by dentists who, having seen the disappointing results of standard orthodontics (cases of facial damage, airway restricting, pain, lack of long-term alignment stability, and so on), have embraced this therapy as a viable alternative.
Forwardontics, like standard orthodontics and dental orthopedics, is concerned with how the teeth are arranged, but it works to correct problems with the teeth in conjunction with those of jaw size and facial structure.
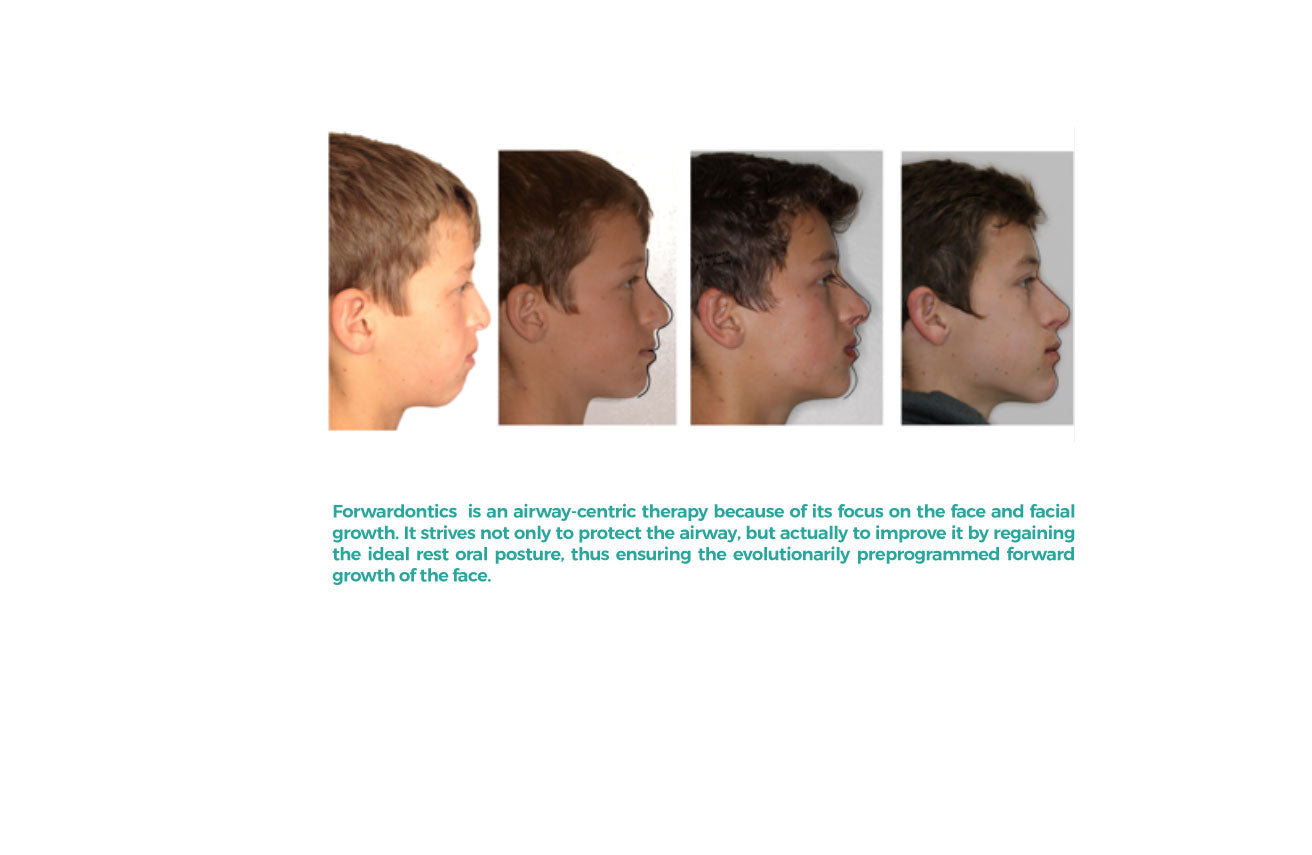
It is especially concerned with avoiding the serious problems that can develop in the airway. Although Forwardontics also uses devices, it works to avoid malocclusion by training people to counter the malign effects associated with aspects of our industrialization (soft foods, spoon feeding, bad body postures, hanging mouth open, etc.) by adopting a healthy oral posture, chewing more thoroughly, reducing nasal congestion, and so on. It works to return the growth pattern of the face to the evolutionary path of our ancestral past.
The Forwardontics choice treatment approach is orthotropics, developed by British surgeon and orthodontist John Mew. In the 1970s, after much experience treating malocclusion and observing how children grow, Mew came up with what he termed the “tropic premise,” (the word tropic referring to growth in response to a stimulus). The tropic premise describes the ideal oral position as “tongue resting on the palate, the lips sealed, and the teeth in light contact for between four and eight hours a day.”
Mew’s basic theories can be easily summarized:
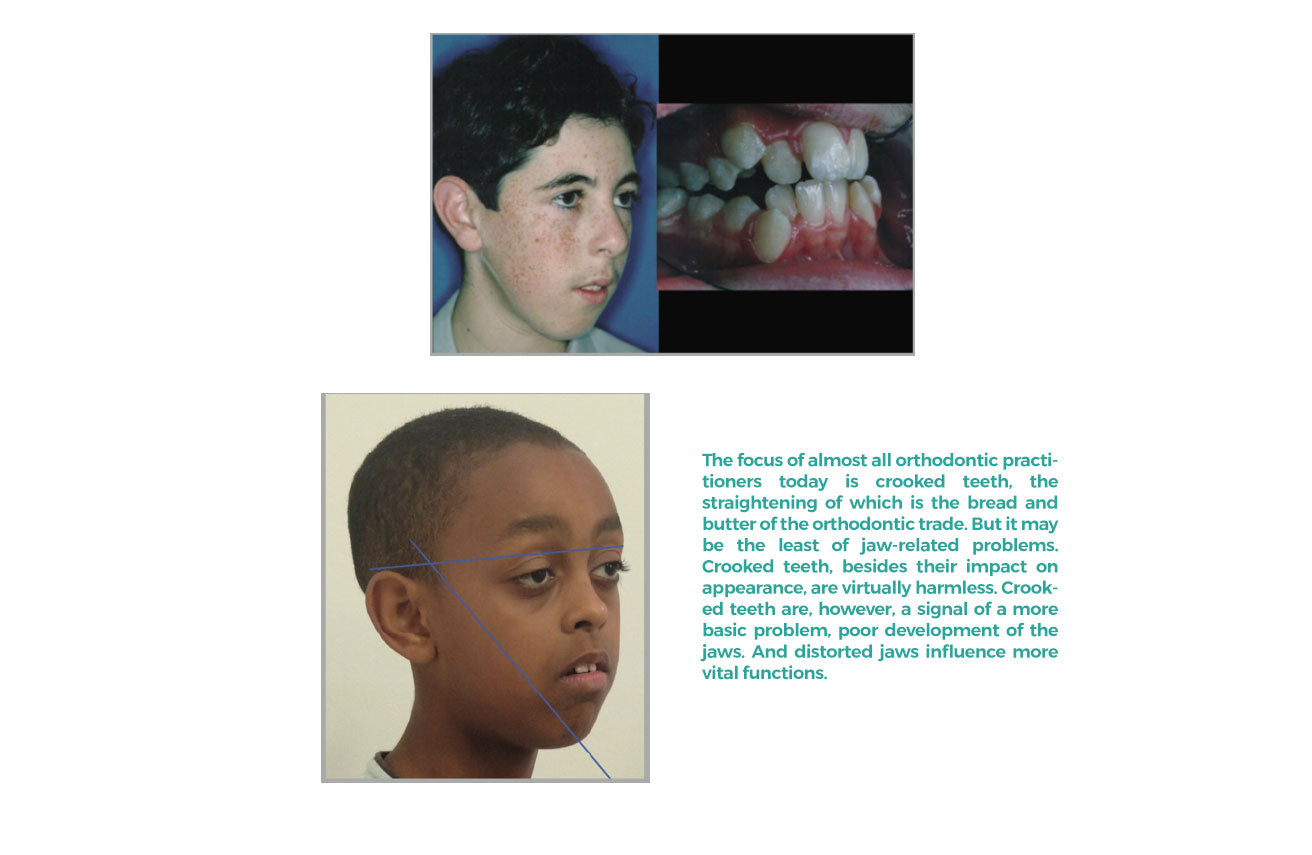
1. In practically every person in modern society both the upper jaw (maxilla) and lower jaw (mandible) are well behind their ideal forward locations for airway development even if the upper jaw appears to protrude.
2. Such underdevelopment of the jaws, as we have seen, is typically a consequence of the person’s eating and breathing history causing an improper interaction between the tongue, the roof of the mouth, and other muscles and bones in the development of the face and jaws.
3. The position of the teeth is not static; teeth keep moving slowly throughout life. Bone is always being dissolved and reformed— reorganized or “remodeled”—contrary to the common impression that it is static and permanent. Thus its shape and the direction that teeth can be gradually moved through it can be changed, this flexibility, the point that bone is not cast like concrete, is the basic fact behind both orthodontics and Forwardontics.
4. This is in line with the general trend of modern medicine to focus on the maintenance of chronic diseases, rather than dealing with their causes.

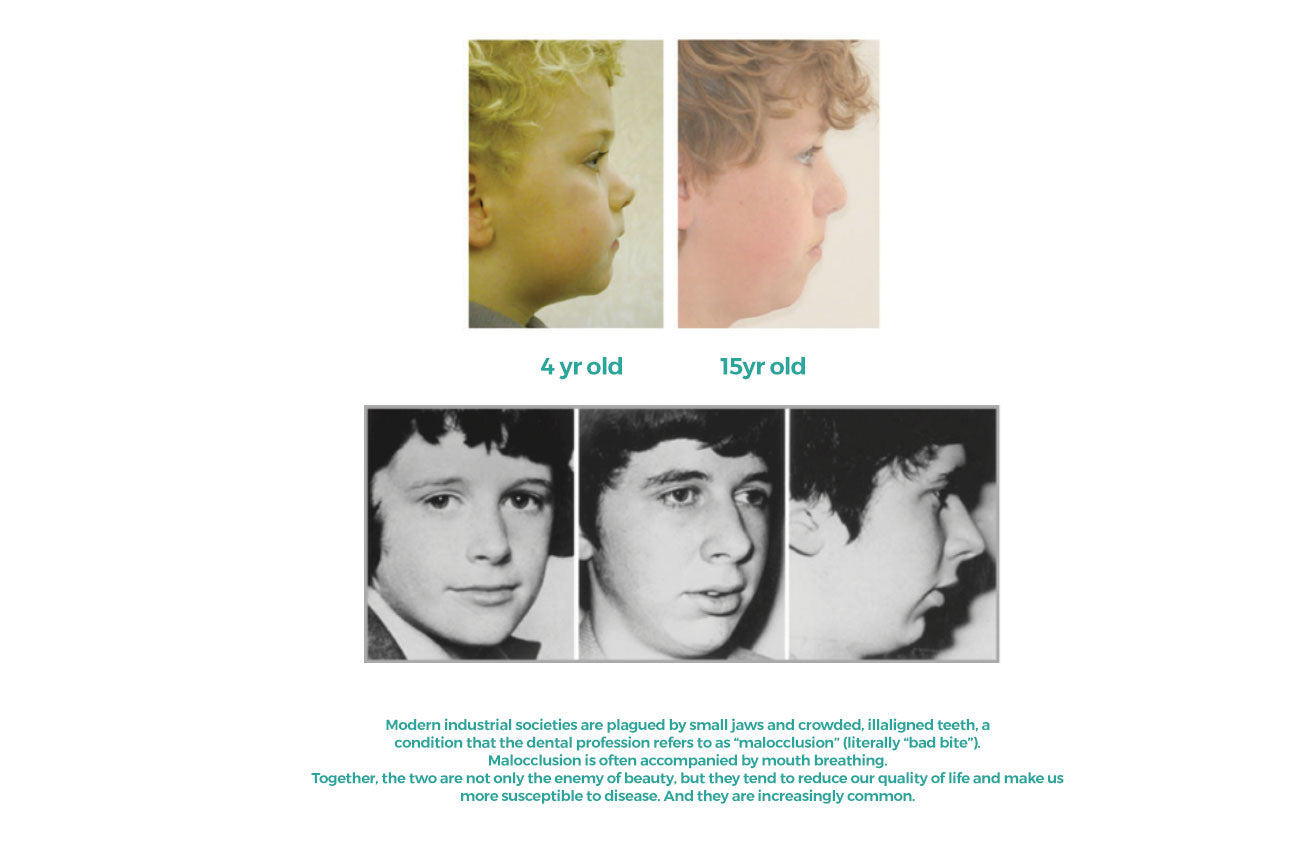
A silent epidemic
How does Forwardontics work?
Forwardontics is designed to prevent malocclusion by guiding growth from an early age, restoring the patterns of chewing pressures and resting posture impacts on muscles and bone typical of traditional human societies. The idea was to keep the mouth closed and to build core strength within the mouth, so that the upper and lower jaws are matched together and growth is symmetrical, balanced, and forward, resulting in a bigger, wider jaw.
Forwardontics utilizes appliances to develop the anatomy (width and length) of the jaws to be able to house the tongue and a healthy airway. Every technique that fosters this “forward” direction is grouped under the umbrella of Forwardontics.
Forwardontics considers the work of muscles, including, but not limited to the tongue, lips and cheeks, toned by appropriate weaning, chewing, breathing, and so forth. Remember, despite casual impressions, the upper jaw is not fixed and would tend to slide back and down without gradual muscular pressure of good oral posture.

Forwardontics and orthopedics: The critical differences
Patients often confuse Forwardontics and dental orthopedics, in part because both emphasize early treatment, but the differences between the two techniques are significant, as are their treatment results. For example, expanding devices for the upper jaw in orthopedics and Forwardontics look similar, but the effects are quite different. Forwardontic expansion is typically more effective and more stable over the long term because of the growth-guiding and behavior modification component of Forwardontics.
In curing malocclusion, the upper jaw almost always needs to be encouraged to move forward, and that is the foundation of Forwardontics. The upper jaw is considered by too many orthodontists to be fixed, which it certainly is not. The upper jaw’s mobility is demonstrated, among other ways, by the very “success” of dental orthopedics in moving it back. Forwardontics focuses on starting treatment in the first decade of life and on widening the upper jaw while moving it up (shrinking the distance between the upper lip and nose) and forward. If the patient maintains proper oral posture, that change will be permanent.